American
![]() f
Manual
Medicine
f
Manual
Medicine
|
American
|
Home
Search
Pain referral
Trigger points
Cranial nerve
Spinal nerve
Historical
About us
Contact us
Site map
The Iliopsoas muscle group is located in the low back and is made up of the Psoas Minor, the Psoas Major, and the Iliacus.
(Absent in approximately 40% of the population).
Anatomical Attachments: Action: Flexes the pelvis and aids in flexion of the lumbar vertebral column.
Nerve Supply: L1 or L2 nerve.
Anatomical Attachments: Action: Flexes the thigh and vertebral column. This is an important postural muscle.
Nerve Supply: Lumbar plexus L2 and L3.
Anatomical Attachments: Action: Flexes the thigh.
Nerve Supply: Femoral Nerve (L2, L3, L4). Synergist: Antagonist: Gluteus maximus, Adductor magnus (posterior part).
Click for Iliopsoas Group Muscle Test
Click for Figure Four Maneuver
Nerve Entrapment: As most practitioners have not been taught to examine the anterior aspect of the iliopsoas or pelvic floor muscles, there is a high prevalence of the population who has low back, hip, abdominal and pelvic symptomatology that is directly related to these two muscle groups. Hypertonicity of the pelvic floor spills over to the iliopsoas; which is frequently observed in tension related myalgia. Persistent hip flexion yields a mechanically shortened iliopsoas, which can be independently tested through the psoas maneuver. In this highly surgerized region of the body, trigger points have the tendency to form in the scar tissue. Therefore, the practitioner is not only assessing for trigger points, nerve compression, reflex pain from visceral disease, but a high preponderance of possible nerve entrapment. Any one or more of the following nerves may become entrapped. Studies devoted to specific syndromes associated with each nerve have not been performed at this time. Therefore, segregation of symptomatology is obscure. The nerves that may become entrapped are the iliohypogastric, ilioinguinal, lateral femoral cutaneous, femoral nerve, obturator nerve, and genitofemoral nerve. Entrapments of these nerves elicit pain or paresthesia in the low back, lower quadrants of the abdomen, pelvis, and genitalia. If the triggers are active in the iliopsoas, they can elicit pain to these same regions, in addition to the hip and superior anterior thigh. As hypertonic muscles give rise to active TrPs, structural deviation, and compressed or impinged nerves and vessels, a practitioner may be presented with a broad array of symptomatology.
Vascular supply: Iliac branch of the iliolumbar artery.
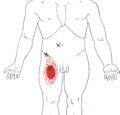
Click on a small image to view an enlarged image Trigger Point Signs and Symptoms: The individual usually sleeps on one side in the fetal position; thus allowing for mechanical shortening of the muscle which reduces low back pressure and discomfort. Upon rising from bed or persistent sitting, low back discomfort is experienced in addition to shortened hamstrings, however, upon walking for a few minutes the low back discomfort and taut hamstrings usually subside. Frequently, low back discomfort is worsened by fecal impaction, which can apply pressure to the triggers in the iliopsoas. As previously stated, the most frequent complaints are that of low back and hip pain, anytime practitioners are confronted with these complaints, or the individual’s inability to perform crunches or sit-ups, they should conduct the Psoas maneuver.
Trigger Point Activating and Perpetuating Factors: Prolonged sitting with their
low back in a jack knifed position (e.g. car riding, truck drivers’ syndrome, and sleeping in a fetal position), stress overload, low back sprain/strain, post surgical adhesions, and increased abdominal girth.
Differential Diagnosis: Quadratus lumborum syndrome, Appendicitis, Degenerative disc disease, (Segmental, Subluxation, Somatic dysfunction) L1 L2 L3 L4 or L5 radiculopathy, S2 or S3 nerve compression, Sciatica, Intervertebral stenosis, Lymphatic cancer, Lymphogranuloma venereum, Neurofibroma, Trochanteric bursitis, Rheumatoid arthritis, Osteoarthritis, Amyloidosis, Cirrhosis, Crohn’s Disease, Colon polyps, Intestinal Obstruction, Irritable bowel syndrome, Leukemia, Surgical adhesions, Systemic Lupus Erythematosus, Aortic aneurysm, Iliac artery aneurysm, Sprain/Strain of the low back, Bone cancer, Bone fracture, Obesity, weakened abdominal muscles, Bladder infection, Kidney cancer, Peritonitis, Kidney stones, Kidney infection, Spontaneous
abortion (Miscarriage), Endometriosis, Ovarian cancer, Ovarian cysts, Pelvic inflammatory disease, Uterine cancer, Prolapsed uterus, Cervicitis, Uterine fibroids, Pregnancy, Menses, Genital herpes, Vaginitis, Vulvitis, Rectocele, Prostrate cancer, Prostatitis, Testicular cancer, Testicular torsion, Epididymitis, Hydrocele, Varicocele, Inguinal hernia, Umbilical hernia, Systemic infections or inflammation, Nutritional inadequacy, Metabolic imbalance, Toxicity, Side effects of medication.
Home
Search
Pain referral
Trigger points
Cranial nerve
Spinal nerve
Historical
About us
Contact us
Site map
Continuing Education © Copyright
Iliopsoas Muscle Group: Psoas Minor, Psoas Major, and Iliacus

Pointer Plus
The Pointer Plus is an easy to use trigger point (TP) locator which
incorporates a push button stimulation feature to immediately treat
Trigger point pain.

![]()
Wireless
Tens Device
Psoas Minor

Psoas Major

Iliacus

Iliopsoas Group
(Psoas Major, Psoas Minor and Iliacus)
Travell and Simons Trigger Point Pain Referral: